TPE for Neurological Disorders: Hope for Patients with MS, GBS, and More
TPE for Neurological Disorders: Hope for Patients with MS, GBS, and More
Neurological disorders, particularly those driven by the immune system, can be devastating. Conditions like Multiple Sclerosis (MS), Guillain-Barré Syndrome (GBS), and Chronic Inflammatory Demyelinating Polyneuropathy (CIDP) often involve the body's own defense system mistakenly attacking the nervous system. This "friendly fire" leads to inflammation, damage to the protective myelin sheath of nerves, and a range of debilitating symptoms from weakness to paralysis.
For decades, Therapeutic Plasma Exchange (TPE), also known as plasmapheresis, has served as a critical lifeline for patients with these conditions. By physically removing the "bad actors"—the autoantibodies and inflammatory mediators—from the blood, TPE can halt the attack on the nervous system and, in many cases, reverse the damage.
In this comprehensive article, we delve into the science behind TPE for neurological disorders, the specific conditions it treats, and the hope it offers to patients seeking recovery and stability.
The Mechanism: Why TPE Works for Neurology
To understand why TPE is effective, we must look at the pathology of autoimmune neurological diseases. In these conditions, the immune system produces autoantibodies. Unlike normal antibodies that fight viruses, these autoantibodies target specific proteins on nerve cells or the myelin sheath (the insulation around nerves).
The Role of TPE:
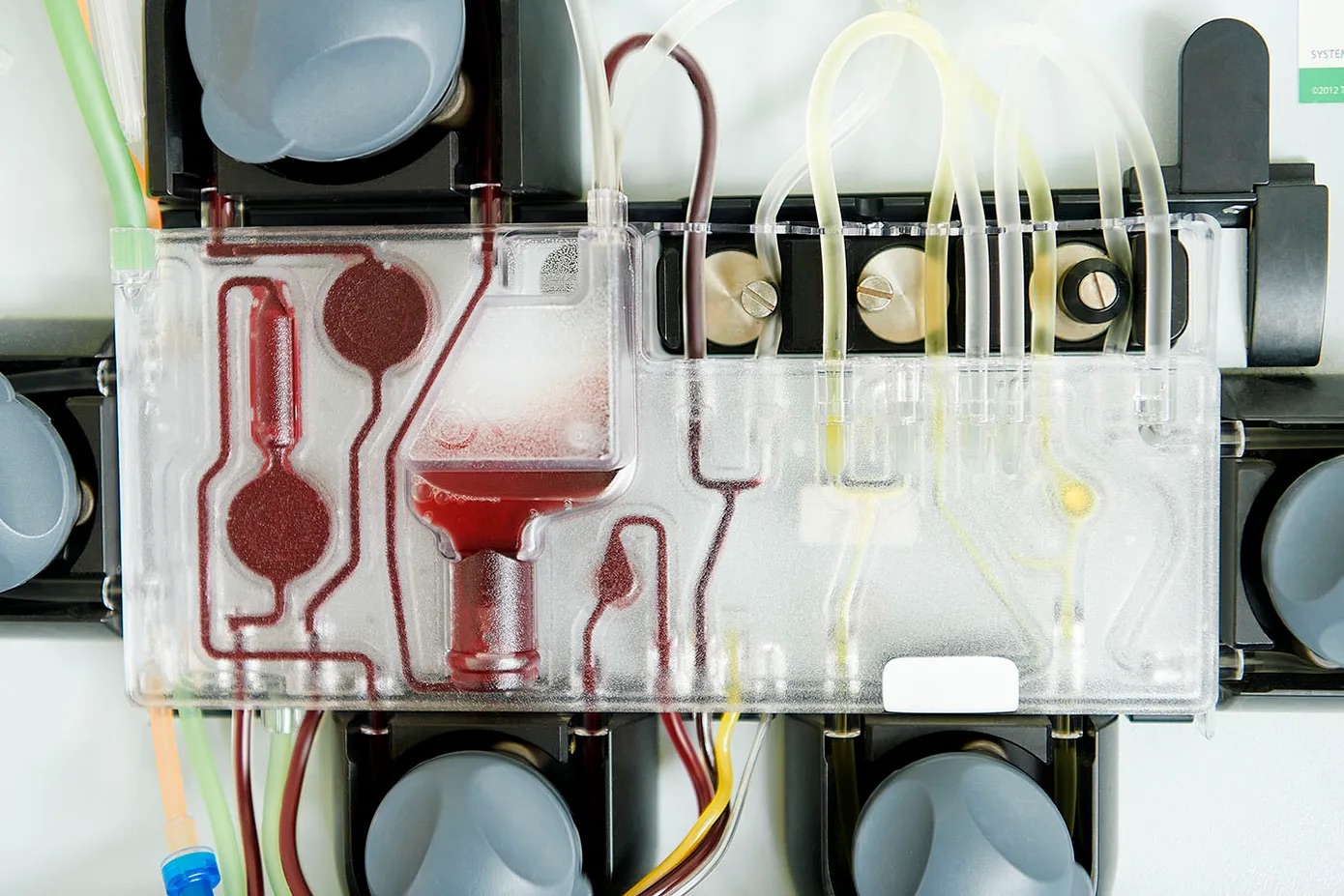
- Removal: TPE works like "dialysis for antibodies." Blood is drawn, separated, and the plasma component containing these harmful autoantibodies is discarded.
- Replacement: The plasma is replaced with a clean fluid (usually albumin), effectively "washing" the blood.
- Reset: By rapidly lowering the load of circulating antibodies, TPE gives the nervous system a chance to heal without constant attack. It also modulates the immune system, potentially making it less aggressive.
Unlike medications that may take weeks to build up in the system, TPE acts immediately. This makes it particularly valuable in acute crises (relapses) or when other treatments have failed.
Key Conditions Treated with TPE
The American Society for Apheresis (ASFA) publishes guidelines categorizing the evidence for TPE in various diseases. For many neurological disorders, TPE is considered a first-line or second-line therapy with strong evidence backing its efficacy.
1. Guillain-Barré Syndrome (GBS)
GBS is a rare, rapid-onset condition where the immune system attacks the peripheral nerves. It often follows a viral infection. Symptoms can progress from weakness in the legs to total paralysis and difficulty breathing within days.
- TPE's Role: TPE is a Category I (first-line) treatment for GBS.
- Impact: Multiple studies have shown that starting TPE within the first week of symptoms significantly speeds up recovery. It reduces the time patients need to be on a ventilator and improves the likelihood of regaining full walking ability after 6 months.
- Protocol: Typically, a course of 5 exchanges over 1-2 weeks is prescribed to clear the antibodies causing the paralysis.
2. Multiple Sclerosis (MS)
MS is a chronic disease of the central nervous system. While TPE is not a cure for chronic MS, it plays a vital role in managing acute attacks (relapses).
- TPE's Role: It is primarily used for acute exacerbations (relapses) that do not respond to high-dose steroids.
- Impact: For patients suffering from a sudden loss of vision, coordination, or strength who fail steroid therapy, TPE can be a "rescue therapy." Studies show that TPE leads to significant clinical improvement in over 40-50% of steroid-resistant relapses.
- Maintenance: In some cases of progressive MS, periodic TPE may help stabilize the disease, though this is less common than its use in acute relapses.
3. Chronic Inflammatory Demyelinating Polyneuropathy (CIDP)
CIDP is essentially the chronic counterpart to GBS. It involves long-term weakness and sensory loss due to nerve damage.
- TPE's Role: TPE is a first-line therapy for CIDP, alongside IVIG (Intravenous Immunoglobulin) and corticosteroids.
- Impact: TPE is highly effective in improving muscle strength and neurological function in the short term.
- Long-term Management: Many CIDP patients rely on "maintenance TPE"—receiving a treatment every few weeks—to keep their symptoms at bay and maintain their quality of life.
4. Myasthenia Gravis (MG)
MG is a neuromuscular disorder causing weakness in the skeletal muscles, often affecting the eyes, face, and swallowing.
- TPE's Role: Used for Myasthenic Crisis (life-threatening breathing weakness) and to prepare patients for thymectomy surgery.
- Impact: TPE rapidly reduces the antibodies attacking the acetylcholine receptors at the neuromuscular junction. It is one of the fastest ways to strengthen a patient in crisis, often showing results within days.
5. Neuromyelitis Optica (NMO)
NMO is a severe demyelinating disease often confused with MS but typically more aggressive, affecting the optic nerves and spinal cord.
- TPE's Role: Evidence suggests TPE is particularly effective for NMO attacks, often more so than in MS. Early initiation of TPE during an attack is crucial for preserving vision and preventing permanent paralysis.
The Patient Experience: What to Expect
Undergoing TPE for a neurological condition can be daunting, but the process is structured and supportive.
- Duration: A typical session lasts 2-3 hours.
- Frequency: For acute conditions (like a GBS or MS relapse), treatments are clustered (e.g., every other day for 5-7 treatments). For chronic maintenance (CIDP), it might be once every 2-4 weeks.
- Vascular Access: Good veins are essential. In acute hospital settings, a central line is often used. In outpatient maintenance, peripheral veins (arms) are preferred if possible.
- Response: Improvement can sometimes be felt after the first few treatments, but often it is cumulative. For nerve damage, healing takes time, so the "antibody removal" stops the damage, allowing the slow process of nerve regeneration to begin.
Conclusion: A Vital Tool in Neurology
For patients facing the frightening prospect of neurological decline, Therapeutic Plasma Exchange offers a powerful mechanism of action: directly removing the cause of the attack. Whether used as an emergency rescue therapy in GBS and MS relapses or as a long-term stabilizer for CIDP, TPE remains a cornerstone of modern neurology.
As research continues, we are also exploring the potential of TPE in neurodegenerative conditions like Alzheimer's, where the removal of misfolded proteins (like amyloid-beta) operates on a similar principle of "cleaning the blood" to protect the brain.
If you or a loved one are battling a neurological autoimmune disorder and standard therapies have not provided relief, TPE may be a viable option. Consult with your neurologist or contact a specialized apheresis center to discuss whether this therapy could be part of your treatment plan.