Transverse Myelitis: Understanding the Attack and the Role of Plasma Exchange

Transverse Myelitis: Understanding the Attack and the Role of Plasma Exchange
The spinal cord is the superhighway of the body. It carries messages from the brain to the limbs ("move your leg") and from the limbs to the brain ("this stove is hot").
In Transverse Myelitis (TM), a section of this superhighway is suddenly bombed.
"Transverse" means extending across the width of the spinal cord. "Myelitis" means inflammation of the myelin (the protective sheath around the nerves). When this inflammation occurs, the messages get blocked. The result is rapid, often terrifying: weakness, numbness, and paralysis that can develop over hours or days.
For patients facing this diagnosis, speed is everything. The standard treatment is high-dose steroids. But what happens when steroids don't work?
This is where Therapeutic Plasma Exchange (TPE) becomes a critical rescue therapy. In this article, we explain the mechanics of TM and why TPE is often the difference between permanent disability and walking again.
What Causes Transverse Myelitis?
TM is an autoimmune phenomenon. The immune system mistakenly attacks the myelin sheath of the spinal cord.
It can be:
- Idiopathic: Happening for no known reason (often post-viral).
- Secondary: Part of a larger disease like Multiple Sclerosis (MS) or Neuromyelitis Optica (NMO).
The attack causes a lesion (a damaged area) on the spinal cord. Depending on where the lesion is (cervical, thoracic, lumbar), the symptoms vary.
- Motor: Weakness or paralysis in legs (and arms if cervical).
- Sensory: Numbness, tingling, or a distinct "band-like" sensation around the torso (the "MS Hug").
- Autonomic: Loss of bladder or bowel control.
The First Line of Defense: Steroids
When a patient arrives at the ER with suspected TM, the first step is an MRI to confirm inflammation and rule out compression (like a slipped disc).
Once confirmed, doctors immediately start IV Solu-Medrol (Methylprednisolone)—high-dose steroids. The goal is to shut down the inflammation chemically.
The Problem: Studies show that steroids alone only result in partial or full recovery in about 50-70% of cases. For the remaining patients, the paralysis persists despite the drugs.
The Second Line: Plasma Exchange (The Rescue)
If a patient does not improve significantly after 3-5 days of high-dose steroids, the standard of care—backed by the American Academy of Neurology—is to initiate Therapeutic Plasma Exchange.
Why TPE Works for TM
Steroids suppress the production of inflammation. TPE removes the cause of the inflammation.
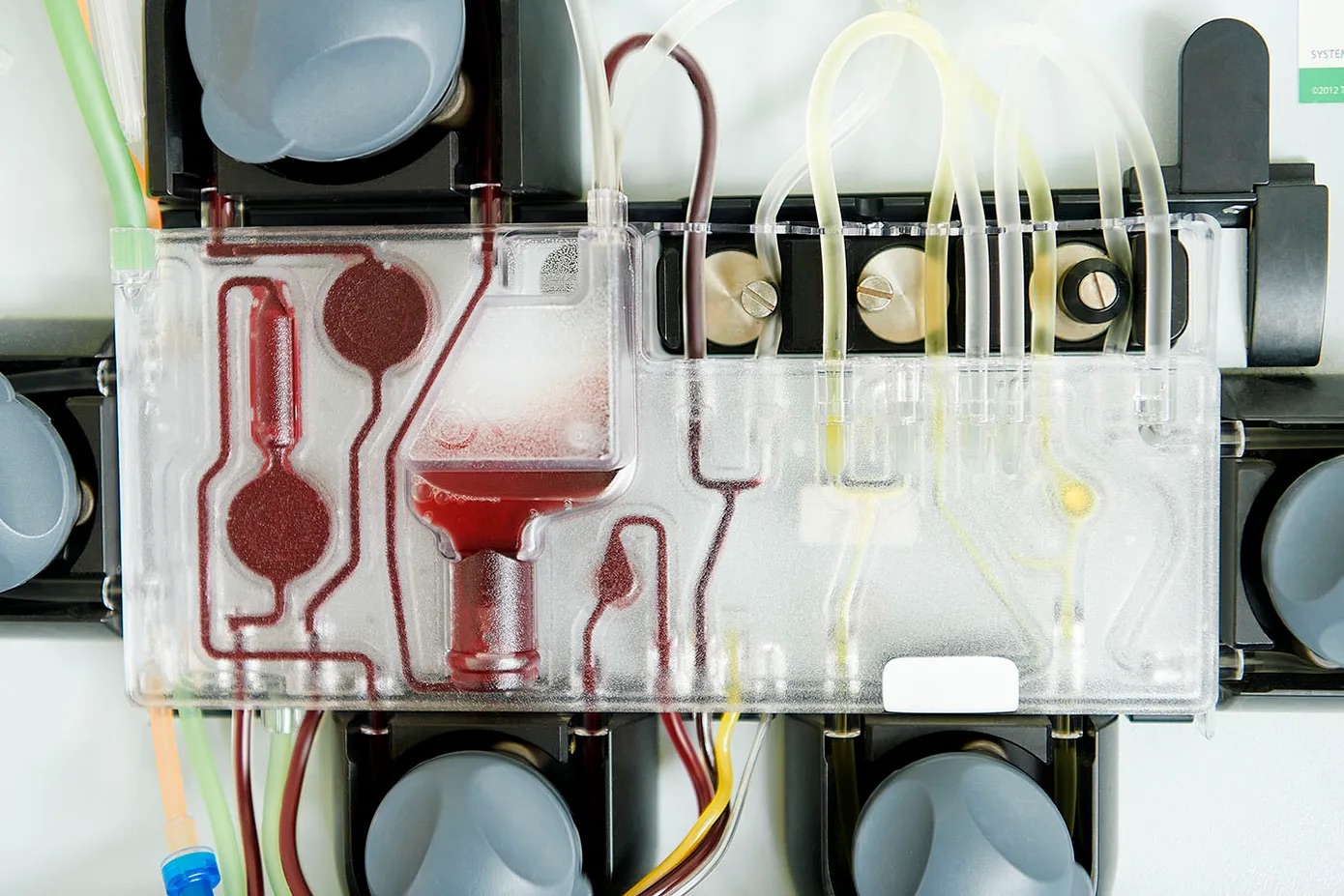
- Mechanism: The attack on the spinal cord is driven by antibodies and cytokines circulating in the blood. TPE filters the blood, physically washing out these inflammatory mediators.
- The "Washout": By removing the antibodies attacking the myelin, TPE stops the active damage. This gives the body a chance to start remyelination (repair).
The Evidence
Research specifically on "steroid-refractory" Transverse Myelitis is compelling.
- A major study found that patients treated with TPE after failing steroids were 4x more likely to have a good functional outcome compared to those who just continued steroids.
- Time Matters: The sooner TPE is started (ideally within 14 days of symptom onset), the better the prognosis. Waiting too long allows the nerve damage to become permanent scarring (gliosis).
The Treatment Protocol
For Transverse Myelitis, the TPE protocol is aggressive because the stakes (paralysis) are high.
- Schedule: 5 sessions performed every other day (e.g., Mon-Wed-Fri-Mon-Wed).
- Volume: 1.0 to 1.5 Plasma Volumes per session.
- Setting: Often started in the hospital. However, if a patient is discharged but still has residual weakness, they may continue outpatient TPE at a clinic like VIP TPE to maximize recovery.
NMO: A Special Case
Neuromyelitis Optica (NMO), or Devic's Disease, is a cousin of MS that causes severe Transverse Myelitis and Optic Neuritis (blindness).
- NMO is caused by a specific antibody: Anti-AQP4.
- These attacks are devastating and do not heal as well as MS attacks.
- TPE is often First-Line for NMO: Because the antibody is so destructive, many neurologists don't wait for steroids to fail. They start TPE immediately alongside steroids to strip the AQP4 antibody from the blood.
Life After the Attack: Rehabilitation and Maintenance
Recovery from TM can take months or years. TPE stops the fire, but physical therapy rebuilds the house.
For patients with recurrent TM (like in MS or NMO), TPE might be used not just for attacks, but as a maintenance therapy to prevent future flares, although newer biologic drugs (Rituximab, Soliris) are often used for prevention.
Conclusion
A diagnosis of Transverse Myelitis is frightening. The sudden loss of function changes life in an instant. But it is important to know that steroids are not the only tool in the box.
If you or a loved one is battling TM and not seeing results with medication, Therapeutic Plasma Exchange is the proven next step. It physically clears the path for recovery.
At VIP TPE, we work with neurologists to provide outpatient TPE for patients recovering from neuro-immunological attacks, ensuring that the window for recovery is kept open as wide as possible.
Learn More: