Therapeutic Plasma Exchange vs. Dialysis: Key Differences Explained

Therapeutic Plasma Exchange vs. Dialysis: Key Differences Explained
In the world of medical treatments that involve "cleaning the blood," two terms often float to the surface: Therapeutic Plasma Exchange (TPE) and Dialysis.
To the untrained eye, they look remarkably similar. Both involve a patient sitting in a chair, connected to a machine via tubes, with blood being drawn, filtered, and returned. This visual similarity often leads to confusion. Patients frequently ask: "Is TPE the same as dialysis?" or "Can TPE help my kidneys like dialysis does?"
The short answer is no. While they share some mechanical principles, they are distinct therapies designed to treat completely different problems. Dialysis is a life-support system for failed kidneys. TPE is a precision tool for removing specific, large, harmful molecules—often related to the immune system—that the kidneys cannot filter out on their own.
In this comprehensive guide, we will dissect the differences between these two powerful therapies, explaining their mechanisms, what they treat, and why knowing the difference could be crucial for your health journey.
The Fundamental Difference: Size Matters
The most critical distinction between TPE and Dialysis lies in what they remove from the blood. This comes down to molecular size.
Dialysis: The Small Molecule Filter
The kidneys are the body's natural filtration system for metabolic waste. When you eat protein, your body produces waste products like urea and creatinine. These are small molecules. The kidneys also regulate water and electrolytes (sodium, potassium).
When kidneys fail (End-Stage Renal Disease or ESRD), these small waste products build up and become toxic. Dialysis acts as an artificial kidney. It uses a semi-permeable membrane to filter out these small molecules and excess water.
- Target: Urea, Creatinine, Potassium, Water.
- Goal: Replace lost kidney function to keep the patient alive.
TPE: The Large Molecule Remover
Therapeutic Plasma Exchange, or Plasmapheresis, operates on a different scale. Many diseases are caused by large molecules—specifically proteins—that are far too big to be filtered by the kidneys or by standard dialysis machines.
These large molecules include:
- Autoantibodies: Rogue immune proteins attacking your own body (as in Lupus, MS, or Myasthenia Gravis).
- Immune Complexes: Clumps of antigens and antibodies that damage tissues.
- Lipoproteins: Cholesterol carriers like Lp(a) or LDL.
- Cryoglobulins: Proteins that clump in the cold.
- Amyloid Beta: The sticky protein associated with Alzheimer's Disease.
Dialysis filters leave these large proteins behind. TPE, however, separates the plasma (the liquid part of the blood) from the cells. It discards the unhealthy plasma—containing all these large, toxic proteins—and replaces it with fresh fluid (usually Albumin).
- Target: Antibodies, Immune Complexes, Lipoproteins, Cytokines.
- Goal: Modulate the immune system or remove specific toxins to halt disease progression.
Comparing the Procedures
While the setup looks similar, the patient experience and the "engine" under the hood differ significantly.
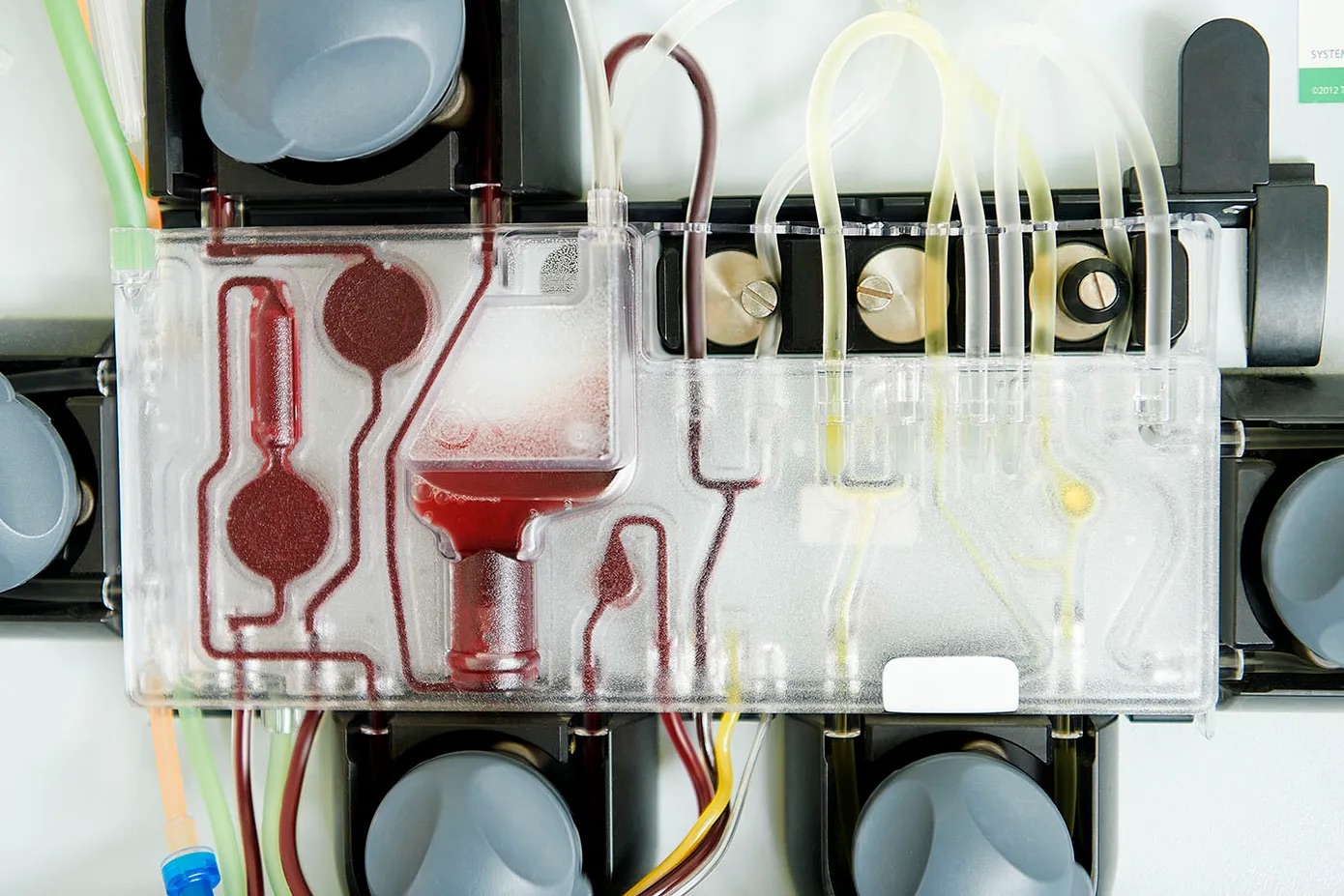
1. The Machine and Mechanism
- Dialysis: Uses a dialyzer (an artificial kidney). Blood flows on one side of a filter, and a special cleaning fluid (dialysate) flows on the other. Physics (diffusion and osmosis) pulls waste from the blood into the dialysate.
- TPE: Uses a centrifuge or a highly specialized filter. The machine spins the blood to separate it by density. Red cells, white cells, and platelets are heavy and sink. Plasma is light and floats. The machine skims off the plasma and discards it. The cells are mixed with fresh albumin and returned to you.
2. Frequency and Duration
- Dialysis: Usually performed 3 times a week, indefinitely, for 3-4 hours per session. It is a chronic, lifelong maintenance therapy unless a kidney transplant occurs.
- TPE: Usually performed as a short-term series (e.g., 5-6 sessions over 2-3 weeks) to treat an acute flare or specific condition. Maintenance might be once a month or once a quarter. It is rarely a daily, lifelong routine in the same way dialysis is.
3. Vascular Access
- Dialysis: Requires a high-flow access point, typically an AV Fistula (surgically connecting an artery and vein) or a graft in the arm. This is a permanent lifeline.
- TPE: Can often be done through standard peripheral IVs in the arms (if veins are good) or a temporary central line (in the neck or chest) for acute cases. It generally does not require the surgical creation of a permanent fistula.
Detailed Comparison Table
| Feature | Hemodialysis | Therapeutic Plasma Exchange (TPE) | | :--- | :--- | :--- | | Primary Goal | Replace kidney function (renal replacement). | Remove specific pathogenic substances (immunomodulation). | | Target Molecules | Small: Urea, Creatinine, Electrolytes, Water. | Large: Antibodies, Immune Complexes, Lipoproteins, Fibrinogen. | | Primary Conditions | Kidney Failure (ESRD), Acute Kidney Injury. | Autoimmune Diseases (MS, GBS, CIDP), Alzheimer's, TTP. | | Fluid Management | Removes excess fluid (ultrafiltration). | Is "Iso-volemic" (fluid removed = fluid replaced). No net fluid loss. | | Replacement Fluid | None (fluid is removed). | Albumin or Fresh Frozen Plasma (FFP). | | Frequency | 3x/week (standard) or daily (peritoneal). | Variable: Daily for acute crisis, then tapered to weekly/monthly. | | Duration | 3-4 hours. | 1.5 - 2.5 hours. |
Can Kidneys Start Working Again After Dialysis?
One of the common questions found in searches is: "Can kidneys start working again after dialysis?"
This depends on the type of kidney failure:
- Acute Kidney Injury (AKI): If the kidneys shut down due to a sudden insult (dehydration, infection, drug toxicity), dialysis may be needed temporarily to keep the patient alive. In these cases, yes, kidneys often recover, and dialysis can be stopped.
- Chronic Kidney Disease (CKD) / ESRD: If the kidneys have slowly failed due to diabetes or high blood pressure over years, the damage is usually permanent (scarring). In this case, kidneys rarely "restart," and dialysis is lifelong.
Where does TPE fit in? Interestingly, TPE is sometimes used to rescue kidneys. In specific autoimmune diseases like Goodpasture's Syndrome or ANCA Vasculitis, antibodies attack the kidneys directly.
- Dialysis cleans the toxins the kidneys can't handle.
- TPE removes the antibodies attacking the kidneys. Used early enough, TPE can sometimes stop the attack and save the kidney function, preventing the need for lifelong dialysis. This highlights the synergy: Dialysis treats the symptom (kidney failure), while TPE treats the cause (autoimmune attack).
Peritoneal Dialysis vs. Hemodialysis vs. TPE
Another common confusion arises with Peritoneal Dialysis (PD).
- Hemodialysis: Blood cleaned outside the body (machine).
- Peritoneal Dialysis: Cleaning fluid is put into the belly (peritoneal cavity). The lining of the belly acts as the filter. Done daily at home.
- TPE: Is strictly an extracorporeal (outside the body) blood procedure. There is no "peritoneal TPE."
Do you live longer with hemodialysis or peritoneal dialysis? Studies generally show similar survival rates, with a slight early advantage for PD. However, neither offers the "rejuvenation" or "anti-aging" potential seen with TPE. TPE is not about surviving organ failure; it is often about optimizing health by removing factors that accelerate aging (like inflammatory cytokines and senescent cell secretions).
Is TPE "Toxic" or Dangerous?
Because TPE involves blood processing, patients ask: "Is TPE toxic to humans?"
The answer is quite the opposite. TPE is a detoxification procedure. It removes toxins. The procedure itself uses sterile, biocompatible tubing. The anticoagulant used (Citrate) is quickly metabolized by the body.
- Safety: TPE is considered safe when performed by experienced teams.
- Side Effects: Most common are mild (tingling from citrate, fatigue). Serious risks (infection, low blood pressure) are rare in outpatient settings.
- "Toxic"? No. The "toxicity" is in your plasma before the exchange. TPE removes it.
For a deep dive into safety, read our guide on Is TPE Safe? Risks and Benefits Explained.
Why VIP TPE Focuses on Plasma Exchange
At VIP TPE, we specialize exclusively in Therapeutic Plasma Exchange. We do not offer dialysis because our mission is not renal replacement, but systemic rejuvenation and immune modulation.
Our patients typically come to us for:
- Neuroprotection: Alzheimer's prevention and cognitive decline (See Early Signs of Alzheimer's).
- Autoimmunity: Managing conditions like Hashimoto's, Lupus, or Neuropathy.
- Longevity: mimicking the effects of "young blood" by removing pro-aging factors (See The Science of Longevity).
Conclusion: Know Your Therapy
Understanding the difference between TPE and Dialysis is empowering.
- If your kidneys have failed, Dialysis is your lifeline.
- If your immune system is attacking you, or if you are seeking to lower your body's burden of age-related toxins, TPE is your solution.
They are different tools for different jobs. In some complex cases (like Myeloma or Vasculitis), a patient might even need both!
If you are exploring TPE for its regenerative or autoimmune benefits, you are in the right place. TPE is a rapidly evolving field offering hope where traditional drug therapies have failed.
Ready to learn more? Check out our FAQ or Contact Us to discuss if you are a candidate for Therapeutic Plasma Exchange.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always consult with your nephrologist or primary care provider regarding kidney failure and dialysis options.